|
|
APPROACHES TO GENE THERAPY
The DNA that genes are made of usually won't penetrate into cells, so it must be somehow transported in. Viruses are the most widely used carriers because they are little more than genes wrapped in a protein coat. But this is a very special protein coat; sticking out of it are specialized proteins that bind to receptors on the surfaces of cells. Once locked in place, they either force their way in or are sucked in by the cell itself.
Some viruses then leave the DNA free-floating in the cytoplasm, while others deliver it into the nucleus, where it is inserted into the chromosome.
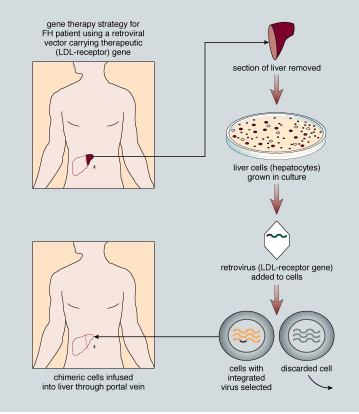
To turn viruses into gene ferries, scientists have developed ways of stripping the genes out of a virus and substituting copies of the genes they want to transfer into cells. The virus is then mixed with cells taken out of the body that are then returned. Or they can be injected directly into the body itself, homing in on the cells of interest. Retroviruses, which insert their genetic code directly into the chromosomes of the host cell, have been used a lot because of their ability to break into chromosomes and insert the DNA. Other viruses are now also being used. One of the big drawbacks of viruses is that the immune system can't tell the difference between bad viruses and those that carry a beneficial gene. So, many of the viruses are rapidly wiped out.
Another approach is to encapsulate the DNA into fatty spheres called liposomes. This approach works because cell membranes are made up of fatty material, and the spheres can simply move across them into the heart of the cell where they release their DNA cargo. Because they're not viruses, they don't touch off a strong immune response, but they also are 10,000 times less efficient at getting the good genes into cells. One idea for improving the efficiency of liposomes is to steal some of those cell-targeting proteins from viruses and plug them into the surface of the spheres. Yet another technique is to simply inject naked DNA. This approach wouldn't work well as direct injection into the bloodstream because the body's DNA-degrading enzymes would quickly digest it. But some experiments have shown that when naked DNA is injected directly into muscle tissue, say, the cells start producing whatever proteins the DNA codes for.
|
|
A CLASSIC CASE AND THE CHALLENGES AHEAD
Andrew Gobea was born in 1993 with what is normally a fatal genetic disease, severe combined immunodeficiency (SCID). This rare disease is thought to strike about one out of every million babies, or a handful of infants in the United States each year. It destroys much of their immune system, particularly the white blood cells called T cells , and leaves the babies defenseless against many life-threatening infections. There are a number of causes for SCID, but, in Andrew's case, he has two defective copies of the gene that codes for a critical enzyme adenosine deaminase (ADA). Without the enzyme, the body fails to break down chemicals produced during normal metabolism that are toxic to T cells. And without T cells, there is no immunity, and with no immunity, death is inevitable. In fact, Andrew's sister Chastity had previously died from SCID, while awaiting a bone marrow transplant that might have saved her life.Because the ADA genes are recessive, his parents had only a one-in-four chance of having another child with SCID. They decided to roll the dice again. Besides learning that Andrew had SCID, Crystal also was told about a bold new medical treatment, which could keep her baby alive-GENE THERAPY. Working copies of the ADA gene could be inserted into T cells, or so doctors hoped. Dr. Donald Kohn, who would perform the gene therapy on Andrew at Children's Hospital in Los Angeles, admits there were doubts and resistance about trying this approach.It was seen as not just a new therapy but a radically new paradigm "putting genes into patients," he saysStill, with a tiny infant's life at stake, Kohn was prepared to step across the threshold and try out this potentially lifesaving therapy.
.The approach he developed was to collect the 100 mL of blood left behind in Andrew's umbilical cord and placenta, which is normally thrown away. This blood, called cord blood, is rich in blood-forming stem cells, identical to those found in bone marrow. Stem cells give rise to a host of blood cells. In fact, cord blood is now being used as a substitute for bone marrow in restoring immune systems. The problem with using Andrew's cord blood was that the cells lacked a functioning ADA gene and were no better than the immune cells he already had. So, Kohn's next task was to insert containing a working ADA gene into these cells. This was no small task. Because DNA will not simply enter cells on its own, Kohn packaged the gene into a virus, which would ferry the new message into the cells. Kohn remembers that day as one of elation and dread. "On the one hand, it's very exciting, and this is what you've prepared for and what you wanted to do. But on the other hand, you worry about failure or, even worse, harming the patient," he says. "This was obviously a momentous occasion; something like this had never really been done. And there's this little newborn with an IV in him that I was pushing the cells into and it was scary."
Some of the cells did indeed take up the gene and began producing T cells with a functioning ADA gene. To insure Andrew's survival, though, he has been given weekly injections of the missing ADA enzyme, at a cost of ,200 a dose. These injections clear the toxic metabolites out of his blood stream and allow the uncorrected T cells to survive.
When Andrew was 18 months old they began tapering off on the amount of enzyme in those injections, to see if the T cells that do produce ADA could take over from those that don't. Now that Andrew is four years old, Kohn asks Crystal if she'll agree to cut off the enzyme altogether. She agrees, but reluctantly.
However, on July 18 it looked like Andrew had caught a cold. A visit to the pediatrician did not provide encouraging news, either. He had thrush, which is a yeast infection of the mouth found commonly in immunocompromised patients. His immune system was crashing and it was time to resume the ADA treatment.
"What we learned from Andrew this summer is that we probably need to get the gene into more cells to have an effect," says Kohn.
This is the challenge that lies ahead for Kohn and other gene therapy pioneers, finding how to get more cells to take up their message and keep producing the enzymes or other proteins that are critical for a patient's health. The quest continues. Using a baseball metaphor, Kohn says, "We are not home yet, but we are at least on third base."
|
|